Restaurant Letter to File a Medical Claim

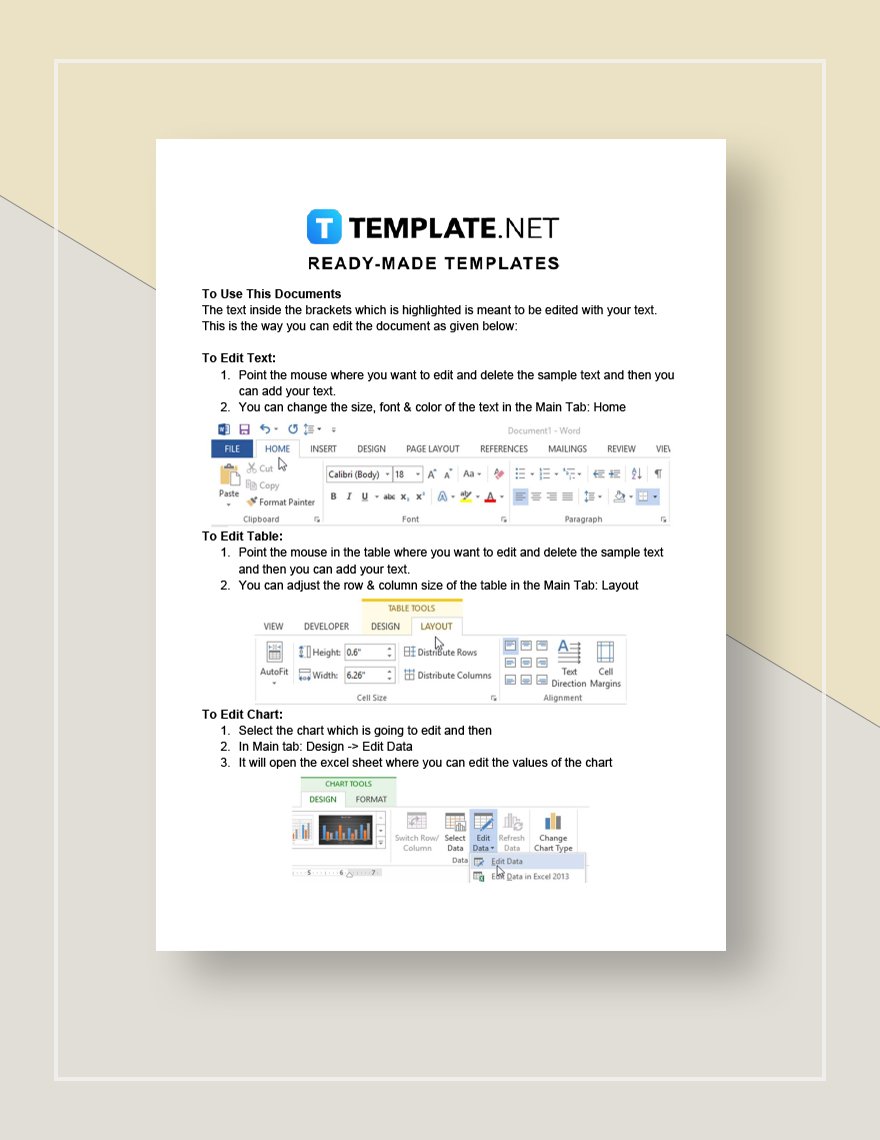
Download this Restaurant Letter to File a Medical Claim Design in Google Docs, Word, PDF, Apple Pages Format. Easily Editable, Printable, Downloadable.
Get to draft a letter to be sent to an insurance company for a health care claim after an incident or injury that took place at a restaurant establishment. To help you draft one, download our premium Restaurant - Letter to File a Medical Claim template. This ready-made file is professionally drafted and easy to use so you can avoid the hassle of starting from scratch. Submit this together with inspection reports, estimates, measurements, notes, and damage assessments to be more effective. This template will surely help you get the job done. Don’t wait for tomorrow. Avail today!
LETTER TO FILE A MEDICAL CLAIM
[SPECIFY NAME OF RESTAURANT EMPLOYEE]
[SPECIFY HOUSE ADDRESS]
[SPECIFY CITY] [SPECIFY ZIP CODE]
[SPECIFY DATE HERE]
[SPECIFY YOUR RESTAURANT NAME]
[SPECIFY COMPLETE STREET ADDRESS]
[SPECIFY CITY] [SPECIFY ZIP CODE]
RE: MEDICAL CLAIM RE [SPECIFY REFERENCE]
Dear [SPECIFY YOUR RESTAURANT NAME]:
I am writing to file a medical claim for the following:
Patient: [SPECIFY NAME OF RESTAURANT EMPLOYEE]
Hospital / Doctor: [SPECIFY NAME OF THE HOSPITAL OR DOCTOR - IN - CHARGE]
Date: [SPECIFY DATE HERE]
As you know, I was on sick leave on [SPECIFY DATE HERE], that day I was hospitalized and take care in [SPECIFY NAME OF THE HOSPITAL OR DOCTOR - IN - CHARGE]. [SPECIFY THE PATIENT’S CONDITIONS AND WHAT HAPPENED]. As a direct and proximate result of my admission, I incurred medical bills, out-of-pocket expenses, lost wages, severe discomfort, anxiety, and pain and suffering. I am submitting my letter to you to avail my medical benefits and such requirements are needed to comply.
The following represent my medical bills and other medical expenses. I have attached copies of representative bills and receipts:
Restaurant Letter to File a Medical Claim
[SPECIFY THE MEDICAL BILLS AND OTHER MEDICAL EXPENSES]
Please approve such request so I can proceed to process my medical claim in the hospital. Thank you and have a good day.
Respectfully,
[SPECIFY SIGNATURE HERE]
[SPECIFY NAME OF RESTAURANT EMPLOYEE]
APPROVED BY:
[SPECIFY SIGNATURE HERE]
[SPECIFY NAME OF THE RESTAURANT MANAGER]
[SPECIFY CONTACT NUMBER]
[SPECIFY EMAIL ADDRESS]
-
Word
-
Google Docs
-
PDF
-
Apple Pages

Already a premium member? Sign in